

By Dan Limmer
I love formative discussions with other educators—the kind that I can’t stop thinking about even after I hang up the phone. I had one of those conversations today.
A friend who teaches for the Army in Texas called me and began the conversation with, “Our students preparing for the NREMT think ‘How much oxygen should this patient get?’ instead of, ‘Should this patient get oxygen?’”
I agreed. We can’t seem to get the oxygen monkey off our backs.
The Wonder Drug Phenomenon
We batted around how to change that thinking. After a bit of discussion, I realized that the American Heart Association changed the oxygen guidelines in 2010, and we still have educators and providers advocating oxygen for every patient. I call this the “wonder drug” phenomenon.
When I speak at conferences and teach my students, I give this example: The next time I treat a patient with anaphylaxis, can I give them 3 or 4 doses of epinephrine with an epinephrine auto-injector? The class is pretty quick to say no. So why do we administer oxygen, a drug capable of doing harm, ignoring any sense of indication or contraindication?
Why? Because we are trying to change an attitude, not a habit. Students don’t come into class thinking oxygen is the wonder drug. We somehow model that for them. Their books don’t say it. The NREMT skill sheets say “high concentration oxygen,” but that is because the patients in the medical and trauma assessment scenarios need it based on indications.
So how do we change this attitude?
Changing How We Think About Oxygen Administration
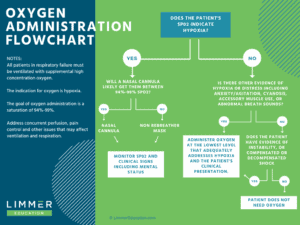
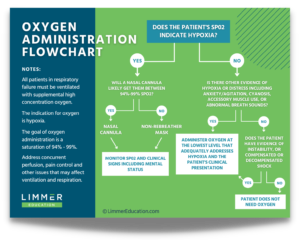 Due to the popularity of this flowchart, we turned it into a glossy 18″ x 24″ poster that you can order for your classroom or station.
Due to the popularity of this flowchart, we turned it into a glossy 18″ x 24″ poster that you can order for your classroom or station.
My answer was that small changes haven’t worked. We need to look at the system that got us to this point and change it. Some ideas include:
- Teaching pharmacology before the airway module in an EMT class. Present oxygen as a drug with indications and contraindications—just like the other drugs they learn.
- Move the pulse oximetry part of the NREMT patient assessment skill sheets up into the primary assessment part of the sheet. If pulse oximetry is part of the decision-making process for oxygen administration, move it to where the student is required to make that decision. Some educators and most students follow those sheets verbatim. At some point, I hope we get away from these practical exams, but that is another topic.
- Make the criteria for oxygen administration clearer to students. There is near universal agreement on the chest pain patient without respiratory distress using the pulse oximeter reading. But what happens if there is also respiratory distress and a saturation of 95%? What if the patient’s skin is moist and their color is poor with a reading of 95%? Let’s not even get into oxygen administration in trauma. That one is all over the board.
Click for larger image
As I typed that last point, the real reason hit me. We might be teaching students, intentionally or inadvertently, to administer oxygen because we ourselves have trouble figuring out when they should and shouldn’t.
Once I realized the issue, I wanted to come up with a solution. I created a flowchart to help put some reason and definition to something we have been struggling with for almost ten years. I’d love to know what you think of it.
There will always be a need for clinical judgment. The flowchart isn’t a recipe or strict guideline. But right now, the target is moving so much it is challenging to teach oxygen delivery. It is challenging for students to learn and apply oxygen concepts to practice (and especially the NREMT). Hopefully, we can change that.
It is time to put this issue to rest. Still.
Oxygen Administration Flowchart Video
Please feel free to share the flowchart with your classes and agencies. We also created a video overview of the oxygen administration flowchart, which you can watch below. We’d love your feedback.


Hi, Dan — LOVE the flowchart & suggestion of moving SaO2 to Primary Assessment, PRN. Keep up the good work!
PS: Any idea when 14th Edition might be out?
The 14th is out! I’m thrilled with the way it turned out. Your Brady rep can get you a copy to review. If you have any problems doing that let me know. Thanks for asking–and for the kind words.
I like it. I think we have both oversimplified AND over complicated the thought process behind giving oxygen. We need to treat it just like the drug it is and I think your flowchart does a nice job of guiding the decision making.
Ruth–I ask people if they would administer epinephrine for anaphylaxis the same way. I don’t exactly know how we got to the stage where we give oxygen until WE feel good. You hit the nail right on the head. As a drug, it has indications and contraindications.
Dan,
After reading your article it inspired me to put in my thoughts behind the oxygen debate. When I was first taught the assessment, the train of thought was; “Everyone gets 15lpm via NRB!” I questioned this fact as to why we were placing such a large amount of oxygen on people who didn’t need it. No clinical evidence would support the notion of high flow oxygen for every patient, only those who showed the signs of requiring the blast of oxygen should receive the treatment. Furthermore, I have noticed many providers at all levels see a non-sustained SPO2 less than 94% without signs of hypoxia immediately grab a NC and throw it on the patient. It seems to me, providers are more focused on treating the tool instead of using sound clinical judgement especially those patients may usually be in the lower 90s due to chronic disease processes. This comes from the skill sheets dictating a hard and fast number to begin treatment, so therefore students are indoctrinated from the beginning to not use clinical judgement. I disagree with moving the SPO2 to the initial assessment, and we should focus on the root issue of improving clinical assessments instead relying on a piece of equipment alone to justify treatment with a medication.
Matt–I sense we have both been out there for some time. You probably recall when a pulse oximeter was giant and cost $1000.00. Back in those days we weren’t particularly trusting of machines and devices telling us what to do. Now a pulse oximeter is $25 on Amazon, almost disposable, and delivered free overnight. I get where you are coming from and don’t believe our positions are mutually exclusive.
Take another device that became small and into our practice some years ago: the blood glucose monitor. Before the appearance of that device, we did the best we could and had a rule, “when in doubt, give glucose.” That wasn’t always good. We have evolved from that. While we know a good history has a place (insulin dose, intake, exercise, vomiting…), we use the BG monitor to help guide our treatment. Interestingly you could still have someone with a diabetic history and altered mental status on the fringe of hypoglycemia where you have to make a decision, but we accept the BG monitor as a valid tool.
Back to pulse oximetry, my issue is that we apply oxygen in the primary assessment. Part of our consideration, based on AHA guidelines, is the pulse oximeter reading. It is fast, relatively accurate, and no one says you have to take away the thinking process. If people are putting it on and applying oxygen rotely based on the reading, that is a training or a QI issue.
I recently was an examiner for an NREMT psychomotor exam. Students who followed the sheet (a.k.a. memorized, which isn’t thinking) put the pulse ox on at the end of the sheet. Guess what? The patient had a reading of 100% (potentially harmful in some conditions) and they have no idea of what it was at the start. A cannula (or sometimes no oxygen) may have been indicated. If you say that treating a patient based on their BG reading + signs and symptoms is ok, why not a pulse oximeter + signs and symptoms? (rhetorical)
Again, I think the part where we are very much in agreement is in the need for thinking. And you aren’t the only person who has called out that we lead with the pulse ox reading. I will also note that things on paper are two dimensional. Things can be done concurrently in practice.
In reality, pulse ox is slapped on early in the call. The AHA helped nudge it in there based on guidelines and I thought that the strength we could give this flowchart is in adding the thinking into practice rather than swimming upstream by denying reality. I hope this makes sense and I am grateful for your comments.
Hi Dan,
I like your flowchart and agree that the NREMT forms need to be updated. Any thoughts about the possibility of CO poisoning?
Angel
Until the NREMT removes the critical failure of performing any part of the secondary assessment before treating threats in the primary this is going to be a persistent issue for educating students and preparing them for their exam. We discuss in lecture numerous times the indications for the application and titrating dose based off of spo2 and presentation, but the nremt removes that critical thinking by mandating it as part of the primary. It would be great if it was treated like any other or drug or treatment in that prior to administration you need to have a set of baselines so you can compare the effectiveness of your treatment.
Cameron–I think that there are probably too many issues with skill sheets and practical exams to mention in one reply. In a reply to a comment above, I noted that you need SpO2 as part of your decision-making for oxygen but the SpO2 is at the end of the sheet with blood glucose.
In another recent experience, a student who takes his practical skills at a remote site said that the instructor didn’t use skill sheets but a prior instructor did. The student liked the skill sheets. I told him that skill sheets are for testing, not learning.
The sad part of this–and the Catch-22 that the NREMT has found themselves in–is if we were to address your issue, there would be people who really didn’t think it was an issue. But they have a different issue. Ultimately the skill sheets might be good for skills check-off during a program but that we are (hopefully) moving out of the final skills evaluation for NREMT certification at some point.
Accreditation has made it so medics have been thoroughly validated on skills. Ultimately you are not alone for a variety of reasons. Thanks for coming by to comment.
If I could give some personal thoughts, knowing full well they are ripe for criticism and assumptions, I’d say this. All angry slanders of my intellectual failures and sands for my patch are welcome.
The flowchart is a decent beginning to a deeper patient assessment and prediction model. It leaves out the most important late stage factor though. (In my uneducated opinion that is).
Patient compensation and predicted progression based on respiratory rate, assumed pH, and if you are feeling fancy (which you should usually) EtCO2 levels. The latter being a safe representative for blood pH and hemoglobins effectiveness at moving and exchanging molecules.
A cardiac patient breathing quickly, perhaps shallow, perhaps deeply, with a saturation reading of 95% we’ll say, and safe to assume anxious even. What we are seeing is a response to a chemical shift in the blood. That’s not news to anyone. But it means our pulse ox becomes less reliable. Alkalosis and acidosis or whatever you call the inching progress towards them, impacts the exchange efficiency and means a hemoglobin, regardless of it’s saturation reading, is performing at a lower level. Exchanging waste and oxygen at a reduced rate. Pair this now with cardiac muscle tissue death and the process of applying an oxygen delivery device (cannula/NRB) and where the patient will be 10 mins from now.
Let’s say this is a STEMI and an EMT from a BLS rig. We see a chest pain, indicating a potential MI, respiratory distress, pale skin (indicating not only reduced oxygenation, but also reduced flow of blood to extremities, yes?) We always say treat the patient not the numbers. They help, but don’t define my treatment.
Stay with me just a little bit longer.
If ideal blood saturation levels are between 94%-99%. We should be shooting for 99%. Given the untrustworthy nature of the assessment tool and ability for a low saturation level to rapidly dip to even lower levels, not to mention we have a patient showing respiratory distress potentially due to a pump problem and thus circulation deficiency (meaning saturation % readings become even more slightly insignificant). A pump issue, we can’t really fix mind you, one with strong potential for sudden and acute decline towards life threatening conditions. We can assume the rapid respiratory rate is in response to pH change of blood, anxiety, and compensation for a failing pump as the body begins to defend against the indicated MI, a condition safely said to be potentially fatal. Would we rather dance between Nasal canula teetering on the line of mild hypoxia from a single tool that has many reasons to be reading a less than useful value, or use a non-rebreather to get the patient to 99% on lower settings with the potential to shift to high values easily given we predict a potential for a sudden decline in the patients condition (prepare for the worst and hope for the best, but we always assume the worst given a defendable reasoning and low risk of doing so). We should include a pH assumption based on EtCO2 as well as recognition of our devices reduced proficiency, paired with not only patient presentation now, but also the chance for patient change soon to come and, should it go less than well, what sort of position we want to be in from an oxygenation standpoint as well as our reason for doing so.
I think it stands to reason the need for not only a teacher/provider/student understanding of the tools and processes at work, but what we should plan for, the risk vs reward of the prevention plan and treatment, as well as the inclusion of all available tools at our disposal to take the most accurate picture this make a more accurate prediction, and considering where you want to ride should the worst (which we usually plan for) should happen. I would want to ride at 99% titrated to patient presentation, supported by multiple tools with an understanding of how the condition effects perfusion and reliability of my tools, and the risk vs reward of my treatment plan, all culminating in an aggressive yet hopefully more precise oxygenation practice that considers all factors and the nuances of a scene as well as the need for simple and withstanding (or as withstanding as we can make it) delivery device to maintain 99% or even more should the patient presentation suggest the need for it. Ultimately eliminating the conditions and factors that cause spo2 errors or untrustworthy numbers, while always respecting the nature of illness and likelihood of threatening drops to the patients wellness, buckling up the seatbelts for suspected turbulence almost, to provide an overarching view and plan that leans towards prepared protection, rather than fear of a few free radicals with minimal risk.
It’s all situational of course, and plenty of scenarios present with 95% sats without any need or benefit, but rather hazard, of oxygen administration. It’s a case by case basis that can benefit from an algorithm, but if I may say with too many words, this one (while being a good start, is not the standing answer to accomplish the knowledge goals and all factors needing consideration.
Ultimately, it probably makes only a small difference if even measurable though. So, to each their own. Great stuff. Always love it. Thanks!
Hi Jacob–That was quite the reply. Here at Limmer Education we are against angry slanders. Things are too crazy now. We need more good. Your comment was thoughtful and we appreciate it.
I won’t post as voluminously and I won’t argue any points. I think your response was thoughtful, pathophysiology-based, and certainly deep. That is where I will start my response. This was designed as a flowchart. The Cliff Notes version. I think there are times when these things are needed. It hits the market, is easy going, and gets people thinking–and hopefully practicing differently.
I also believe that a majority of the market is at the EMT level. While I don’t think EMTs always get the patho they should in class, this flowchart helps them understand or appreciate decision-making about oxygen at basic and functional cognitive levels.
Finally, I think your reasoning is the dotted line, the thinking in the space between the sections in the flowchart, that people get in class or sometimes learn on their own as they begin to practice. Coming full circle, there is a place for flowcharts and a place for detail.
I hope people take the time to read your thoughtful post.
I feel most instructors agree with appropriate oxygen usage. However, when will the NREMT stop with the “pigeon-hole” mentality of “high flow oxygen” on the exams? We all dislike teaching a skill or knowledge point, but only to qualify it with “but on the NREMT exam, you do X”. The NREMT is making changes , but until then…our students still struggle.