

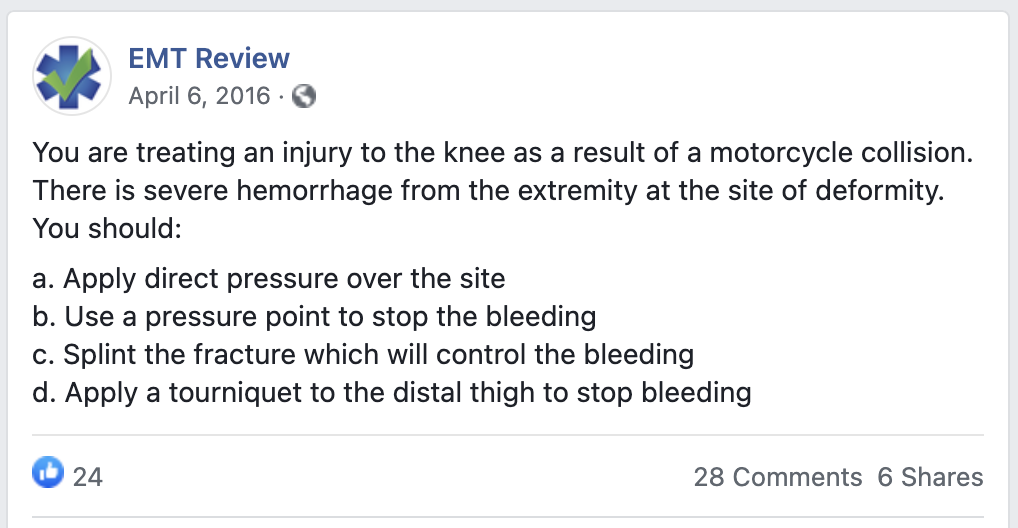
A recent post on our EMT Review Facebook page was one of our favorites because of the discussion that ensued—thank you to everyone who participated. If you didn’t see it, here’s the question posted:
Linear Thinking in Bleeding Control
We will warn you that we love questions like this because they highlight the hazards of linear thinking in EMS—the belief that there’s one set way to apply the rules learned in class.
A small distinction is very important here. There are many ways to apply the concepts learned in class and that all of them are correct. As a matter of fact, this is what distinguishes the students who end up “getting it” from those who don’t.
Let’s look at the choices in the question:
a. Direct pressure. This is the traditional first step in bleeding control. Direct pressure might stop the bleeding, but it also would cause immense pain and potentially further vascular and nerve damage in a joint known for potentially serious vascular and nerve issues.
b. Pressure points. This answer isn’t an option, according to the latest trauma guidelines. There is no proof that using pressure points works—and there’s no time to waste with a severe hemorrhage.
c. Splinting. This might slow bleeding and will prevent further injury, but splinting is not a primary method of bleeding control.
d. Tourniquet. This will stop the bleeding, but will it do harm?
The value of this question lies in its realism: the way it mimics the street, where often there are no great answers, so you have to make the best choice. Hemostatic agents aren’t listed as a choice, but they might be an option.
Turning Linear Steps into Guiding Principles
So how do we bridge the gap between classroom-based concepts and scenario-based multiple choice exams—and the street? Let’s look at the basic rules we’re taught:
- We’ve been given set guidelines for bleeding control—basically, apply direct pressure first, then tourniquet.
- We’ve been told to minimize the movement of fractures by splinting them. Movement other than for necessary realignment is bad.
- In medicine, we should first do no harm.
If we take these rigid steps and transform them into guiding principles, the path seems clearer.
In this scenario, we would apply a tourniquet. Few locations are so remote that an EMT couldn’t get to a hospital in time to deal with the bleeding and save the limb (assuming it could be saved in the first place). This would spare the patient additional damage and tremendous pain. The choice here rests on a risk-benefit ratio—plus, with a motorcycle crash, we’d want to get moving anyway.
The 8th edition of PHTLS (p. 234) says:
Tourniquets had fallen out of favor because of concern about potential complications including damage to nerves and blood vessels and potential loss of the limb if the tourniquet is left on too long. None of these have been proven and, in fact, data from the Iraq and Afghanistan wars have demonstrated just the opposite.
What do you think? Should you apply pressure because that is the “first step”? Do you believe the risks involved in tourniquet application are more than or less than those of applying direct pressure over a deformed knee?
Answering questions like these is what EMS thinking is truly about—and what education should prepare students to do. It is much different from teaching the steps to control bleeding by following a skill sheet.
In my opinion the answer is D. 12 years of combat medicine has demonstrated that it does minimal harm provided the patient can be packaged and transported to a trauma center quickly. I don’t get a lot of trauma calls in my area but I still carry a tourniquet in my pocket.
Are you basing that the correct answer is D because that is what the NREMT would have as the correct answer or because that is what is correct based on data and real world experience? I am just wondering because isn’t this site’s intention to help people pass the NREMT? So wouldn’t all of your questions and correct answers be what the NREMT would have as the correct answer?
Gary–I think there is a common false belief that the NREMT has some sort of secret medicine different than the book or real life. This isn’t true. While the questions are a different type than many see in class, it is all based on the same science.
For the NREMT you will pick the best answer. This doesn’t mean the correct answer. The BEST answer. It tests your judgment in a situation rather than the recall of facts. In the question above can you see how the tourniquet is the best answer? It doesn’t cause harm (like direct pressure could) and it acts promptly (as the splint doesn’t) and pressure points are out of our mainstream toolbox for bleeding control–especially with severe hemorrhage. This would pass several tests: current science, what I’d want if it were my leg and I believe the NREMT as well.
I hope this helps!
My class was taught by an EMT/RN with 20 years experience. We were taught tourniquet as last resort, just like in the book and now you say Nremt has Tourniquet as the answer? There is something wrong at Nremt
Tony–When you go through a class you spend a lot of time with your instructor and in most cases you hold that instructor in high regard forever. I respect the experience of your instructor.
I will however disagree with the “tourniquet as a last resort” statement. It doesn’t match the intent of the scope of the current science in regard to bleeding control. A severe bleed can cause death in 2 – 4 minutes depending on the location. There are times when you will switch to a tourniquet quickly because it is effective and direct pressure doesn’t work quickly enough. This is supported by science and the trauma books.
You may also go to a tourniquet in other situations. Perhaps you have multiple patients and you want to stop bleeding quickly and free yourself up to treat other critical patients. In this case is it better to put direct pressure on the deformed going and risk other damage? (See my response above for more details).
There are few rules in the street (and the NREMT) that are held to absolutely. Everything is a judgment based on what you have before you. Best to you on the exam. Let me know if you have additional questions.
This is an excellent question, but it does present a difficult conundrum.
While you accurately quoted from PHTLS 8th Ed.; the beginning sentence of that paragraph is, “If external bleeding from an extremity cannot be controlled by pressure, application of a tourniquet is the reasonable next step in hemorrhage control.”
Any quotation from a text taken out of context can support nearly any position.
That said, I agree that the application of a tourniquet as the first line in bleeding control in this scenario is proper as a field intervention, I have difficulty in the classroom (and on an exam) with this sequence of treatment.
Hi Jay. I’ll start by saying you aren’t alone. If you read my responses to the posts above you’ll see that the answer to these and many questions are truly “between the lines” of all the sources. I personally wish we could just give guidelines instead of steps. While it may be more stressful to students learning a skill initially (and for educators teaching it), it would be better for the NREMT and practice. Something like this for bleeding control:
1. Do no harm. If this isn’t possible, do the least harm you can always in the patient’s best interests.
2. Don’t let the patient bleed to death. In severe bleeding (or more minor bleeding combined with bleeding in other places), hemorrhage must be stopped quickly by the most appropriate means.
3. The general techniques of bleeding control (direct pressure, hemostatic agents and tourniquet) will be used in a manner consistent with the patient’s clinical picture.
4. Situations that may cause you to alter your care include multiple patients, multiple critical situations in the same patient, the location of the bleeding, other injuries to the same areas of the body and more.
It is best to stop thinking of things as “rules” and consider it a toolbox where clinical judgment (under stress) is where the decisions are made on what is best to take from the toolbox in any given situation.
Thanks for the question.
Hi Dan. Hope to be in your neck of the woods soon! (My family is from the Pemaquid region)
I really think we are singing in unison on the question, we met at a 91W Educators’ conference in San Antonio years ago, so I’m right there with you on the rapid application of the tourniquet in this scenario.
I guess what I’m differing with you on here is the nature of the item and the assumption that following standard practice (beginning with direct pressure) is not the best answer when provided with these distractors.
When I was on the EMT-I85 test item writing group with NREMT, Gregg Margolis kept drilling it into us, “this is a test, not a teaching tool.” He would guide us away from questions that provided more of a opportunity to “read into the question” rather than provide an opportunity to recall accepted practice. Now know that scenario based questions and critical thinking were encouraged in items and I don’t presume to put words in Gregg’s mouth.
I too want to be able to lay out guidelines rather than steps (which is why I’m turning to places like Ireland) and do so in regular simulated cases with psychomotor and affective objectives that outweigh the cognitive in evaluation. We need to start admitting that technical proficiency is not the end point of our education programs, but the starting point. HOW we perform is important, but no where near as important as WHY and WHEN.
I just realized I mess up in that post. I meant to say that in simulation cognitive and affective objectives outweigh the psychomotor.
“If external bleeding from an extremity cannot be controlled by pressure, application of a tourniquet is the reasonable next step in hemorrhage control.”
Even with the text it is very clear. In this scenario, the bleeding couldn’t be stopped with direct pressure as it is on a joint. The responder doesn’t have to attempt direct pressure in this case to know that it would be futile therefore jumping to the next step is the best option.
“In this scenario, we would apply a tourniquet. . . . This would spare the patient additional damage and tremendous pain.”
It is not evident to me from the question that the nature of the injury is such that direct pressure would cause “additional damage and tremendous pain”. (If it were, I would agree with you that you would go straight to the tourniquet.) What am I missing here?